
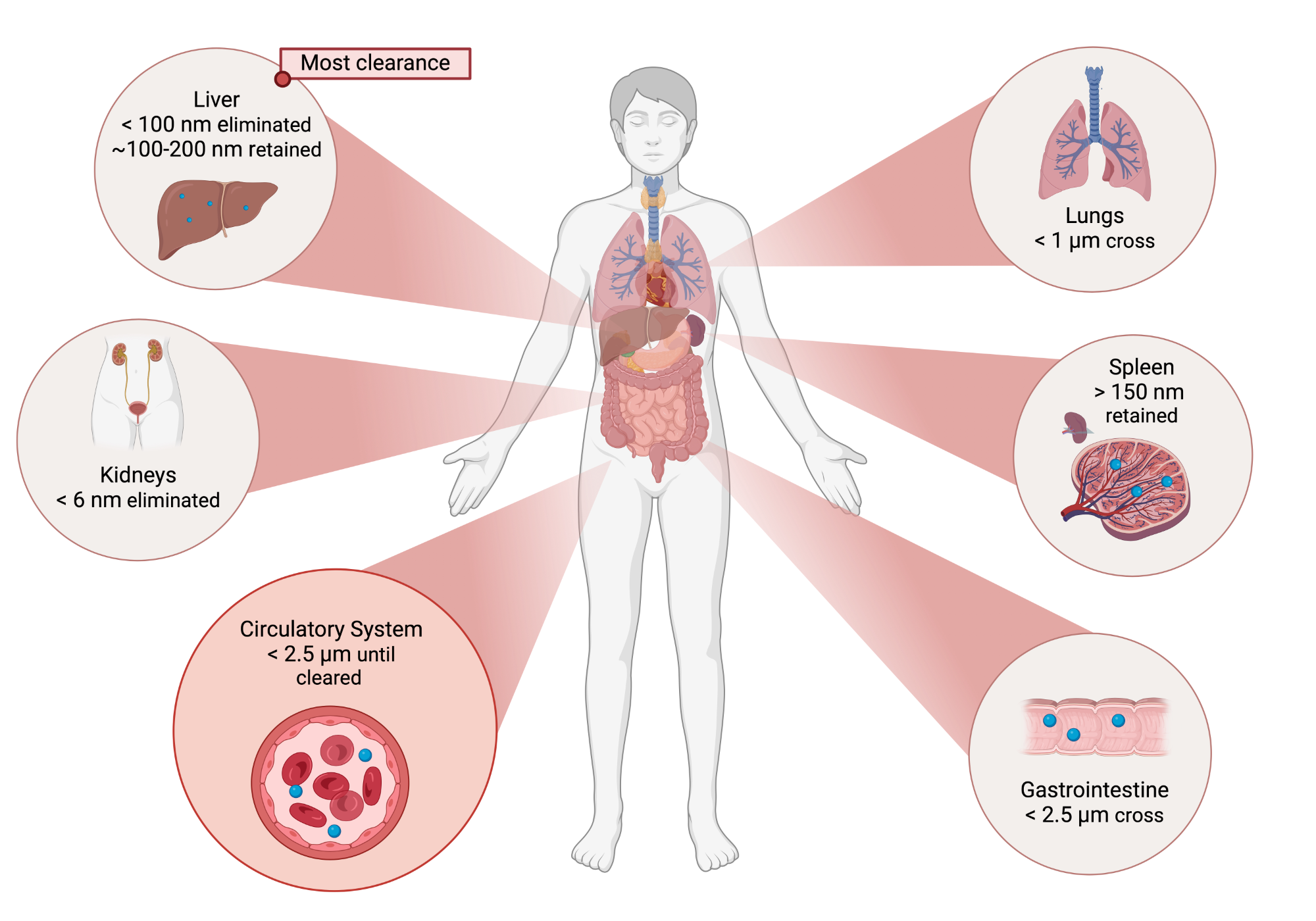

Once ingested, particles smaller than 2.5 μm can enter the gastrointestinal tract through endocytosis and enter the circulatory system. (2,3) Airborne particles smaller than 10 μm can be inhaled through to the terminal branches and alveolar air sacs of human airways (3) and particles smaller than 1 μm (nanoparticles) have the potential to cross lung tissue barriers and also enter the circulatory system. (2) As the smallest internal diameter of capillaries are typically ∼7–17 μm, (4) only very small micron or nanosized particles can be transported through the body. Once in the bloodstream, particles smaller than ∼6 nm are rapidly eliminated through the kidneys via urinary excretion (5,6) while larger particles can be cleared from circulation by the mononuclear phagocyte system (MPS) (7) through sequestration in the liver and spleen. (5) The majority of particle clearance occurs within the liver with an estimated removal of 30–99% of nanoparticles in the bloodstream (5) although this is dependent on particle properties such as size and charge. Particles that are not taken up by the liver may be cleared by the liver during subsequent passes. (8) Within the liver, particles >100 nm can be retained long-term within Kupffer cells (6) whereas smaller particles (5) can pass into the space of Disse for excretion via the biliary pathway for eventual elimination in the feces. (6) The spleen is the largest blood filtering organ in the body, eliminating particles >150 nm (9) with splenic uptake increasing with particle size. (9) Uptake to spleen macrophages is significantly reduced as compared to Kupffer cells. (8) Certain medical conditions can increase the presence of barrier cells which work in conjunction with macrophages to increase clearance (9) or create leaky barriers allowing increased migration. (10)See full article for references.
